
by James D. Agresti
Roughly two-thirds of U.S. residents don’t believe the CDC’s official tally for the number of Covid-19 deaths. This distrust, however, flows in opposing directions. A nationally representative survey conducted by Axios/Ipsos in late July 2020 found that 37% of adults think the real number of C-19 fatalities in the U.S. is lower than reported, while 31% think the true death toll is greater than reported.
The facts show that neither side has an airtight case, but the evidence is more consistent with the theory that less people have died from C-19 than the official figures indicate. Nevertheless, the extent of the possible overcount is unknown, and even if it were as high as 50,000, it would not make a marked difference in key measures of the pandemic’s severity. Hence, debates over the accuracy of the death toll distract from other issues with much greater implications.
Excess Deaths
The main argument of those who claim that the official C-19 death tally is an undercount is based on a factor called “excess deaths.” This is defined as the total number of deaths from all causes during the pandemic minus the number of deaths that would normally occur at this time of the year.
In the words of the Government Accountability Office, “Examining higher-than-expected deaths from all causes helps to address limitations in the reporting of Covid-19 deaths because the number of total deaths is likely more accurate than the numbers of deaths from specific causes.”
U.S. death certificate data shows that the rise in deaths during the pandemic has indeed been greater than the number of reported C-19 deaths. Some jump to the conclusion that these additional fatalities must be C-19 deaths that were not recorded as such, but a broad array of data indicates that the bulk or all of them are caused by societal reactions to C-19—instead of the disease itself.
For a prime example of how people misconstrue this issue, CNN’s chief media correspondent, Brian Stelter, reported on August 16:
We are likely to see the 170,000 mark crossed today—confirmed deaths from Covid-19. But researchers have looked at the actual number of excess deaths in this country—estimated deaths above the norm—and they say it’s closer to 200,000 so far this year. So the real actual death toll from Covid-19 is around 200,000. We have to constantly remind viewers that it’s even worse than we know. It’s even worse than the data indicate.
First, Stelter is wrong that this figure is for “confirmed” deaths. It is actually for “confirmed” plus “suspected” deaths. Those exact words come from the CDC’s official guidance for certifying C-19 deaths, which was published on April 3. On the same day Stelter made this claim, the CDC’s website stated that its C-19 “case counts and death counts” have included “both confirmed and probable cases and deaths” since April 14. In other words, Stelter misrepresented the essence of the data even though this accounting change was in effect for four full months.
The impact of including probable deaths in the count is evidenced by how the CDC altered its website when it adopted this methodology. Two days after the new method of counting deaths was implemented, the CDC updated its website twice (instead of its usual once-per-day update) to incorporate this revision. The changes it made on that day (April 16) provide a rough sense of scale for how the new policy modified the death toll:
- Before any updates, the CDC reported that 24,582 people had died from C-19 as of April 14.
- On the first update, the CDC reported that 27,012 people had died from C-19 as of April 15, including 22,871 “confirmed” and 4,141 “probable.”
- On the second update, the CDC reported that 31,071 people had died from C-19 as of April 15, including 26,930 “confirmed” and 4,141 “probable.”
Taken at face value, the second update shows that CDC’s insertion of “probable” cases raised the death count from 26,930 to 31,071, or by 15%. From a more skeptical standpoint, the difference between the 22,871 “confirmed” deaths on the first update and the 31,071 “confirmed and probable” deaths on the second update amounts to a 36% rise caused by these bookkeeping modifications.
More significantly, Stelter failed to reveal that scholars who conduct research on excess deaths have found that multitudes of them have been caused by lockdowns, panic, and other responses to the pandemic. In July 2020, the Journal of the American Medical Association published a paper regarding this matter by researchers from Virginia Commonwealth University and Yale University. An article about the study from Virginia Commonwealth University summarizes its findings and quotes the researchers as follows:
- Some excess deaths “may reflect under-reporting” or “patients with Covid-19 who died from related complications,” “but a third possibility, the one we’re quite concerned about is” the “spillover effects of the pandemic, such as delayed medical care, economic hardship or emotional distress.”
- In the five states that that had the most Covid-19 deaths in March and April:
- stroke deaths were 35% above normal.
- Alzheimer’s deaths were 64% above normal.
- heart disease deaths were 89% above normal.
- diabetes deaths were 96% above normal.
- “New York City’s death rates alone rose a staggering 398% from heart disease and 356% from diabetes.”
- “Still others may have struggled to deal with the consequences of job loss or social isolation.”
- “A number of people struggling with depression, addiction and very difficult economic conditions caused by lockdowns may have become increasingly desperate, and some may have died by suicide. People addicted to opioids and other drugs may have overdosed.”
- “The findings from” the “study confirm an alarming trend across the U.S., where community members experiencing a health emergency are staying home—a decision that can have long-term, and sometimes fatal, consequences.”
Numerous other facts corroborate the ones above, a small sampling of which includes the following:
- A scientific survey commissioned by the American College of Emergency Physicians in April 2020 found that 29% of adults have “actively delayed or avoided seeking medical care due to concerns about contracting” C-19.
- A California-based ABC News station reported in May:
- “Doctors at John Muir Medical Center in Walnut Creek say they have seen more deaths by suicide during this quarantine period than deaths from the Covid-19 virus.”
- Mike deBoisblanc, head of the trauma unit at the hospital stated that he’s “seen a year’s worth of suicide attempts in the last four weeks,” and “mental health is suffering so much” that he says “it is time to end the shelter-in-place order.”
- A scientific survey conducted by the CDC in July 2020 found that about 32% of U.S. adults had “symptoms of anxiety disorder” as compared to 8% around the same time last year. The perils of this are underscored by a 2015 meta-analysis in the Journal of the American Medical Association Psychiatry, which found that the overall risk of death among people with anxiety is 43% higher than the general population.
- A study published by the American Medical Association in September 2020 found that 27.8% of U.S. adults had symptoms of depression during the C-19 pandemic as compared to 8.5% before the pandemic. The same 2015 meta-analysis found that depression is associated with a 71% higher risk of death.
- An article published by the Federal Reserve Bank of San Francisco estimated that “more than 20 million jobs” were “swept away” in the early months of the C-19 pandemic. A 2011 meta-analysis in the journal Social Science & Medicine about mortality, “psychosocial stress,” and job losses found that “unemployment is associated with a 63% higher risk of mortality in studies controlling for covariates.”
- A study published by Just Facts in May 2020 found that anxiety related to C-19 will ultimately destroy at least seven times more years of life than can possibly be saved by lockdowns. With regard to this study, the accomplished psychiatrist Joseph P. Damore, Jr. wrote that it “thoroughly answers the question about the cure being worse than the disease.”
Thus, many or all of the excess deaths that Stelter and others attribute to C-19 are caused by the actions of governments and media outlets. These include but are not limited to stay-at-home orders, business shutdowns, and pervasive misinformation that fuels ill-informed decisions, panic, and depression.
Evidence of Overcounting
Several lines of evidence prove that some deaths included in the official C-19 tally were, in fact, not caused by C-19. However, the combined weight of this evidence is not enough to prove that the reported death toll is significantly greater than the actual one.
Four weeks after the World Health Organization declared C-19 a pandemic, Dr. Deborah Birx, the coordinator of the White House Covid-19 task force, stated that the U.S. is taking a “a very liberal approach” to counting C-19 deaths compared to “some countries.” She then explained that “if someone dies with Covid-19, we are counting that as a Covid-19 death.” Notably, that standard does not distinguish between dying from Covid-19 and dying with Covid-19.
In the wake of Birx’s statement, various government officials revealed exactly how they were implementing this “very liberal approach”:
- A Michigan news article reported in April:
-
- “In Macomb County, Chief Medical Examiner Daniel Spitz had a recent case in which an individual died by suicide. Because they had a family member in the hospital suffering from Covid-19, Spitz had a postmortem test done and found that the individual who died at home was positive for Covid-19. The virus wasn’t their cause of death, but the individual is counted as a Covid-19 death.”
- In Oakland County, “every individual who has died while infected with Covid-19 has counted as a coronavirus death, according to Dr. Ljubisa J. Dragovic, the county’s chief medical examiner.”
- Ngozi Ezike, director of Illinois Department of Public Health stated during a April press conference:
-
- If “you were in hospice and had already been given a few weeks to live, and then you were also found to have Covid, that would be counted as a Covid death. It means that technically, even if you died of a clear alternate cause, but you still had Covid at the time, it’s still listed as a Covid death.”
- “So everyone who’s listed as a Covid death doesn’t mean that was the cause of the death, but they had Covid at the time of death.”
- A month later, Ezike said that the Department of Public Health was partly unwinding its previous policy but some of it would remain in place:
-
- We are “trying to remove those obvious cases” from the C-19 death tally “where the Covid diagnosis was not the reason for the death. If there was a gunshot wound, if there was a motor vehicle accident, we know that that was not related to the Covid positive status.”
- If “someone has another illness, like heart disease, and then had a stroke or other event, it’s not as easy to separate that and say Covid didn’t exacerbate that existing illness. That would not be removed from the count.”
- “Even if somebody was very elderly and they were maybe in hospice, we still can’t say that their Covid infection didn’t hasten the death, and so it’s relevant that Covid-19 maybe had a chance to accelerate that process.”
- A Colorado-based CBS news station reported in April:
- The “Colorado Department of Public Health and Environment has reclassified three deaths at a Centennial nursing home as Covid-19 deaths, despite the fact attending physicians ruled all three were not related to coronavirus.”
- A spokesman for the state explained that it “follows the CDC’s case definition of Covid-19 cases and deaths,” and “when a person with a lab-confirmed case of Covid-19 dies, their death is automatically counted as a Covid-19 death unless there is another cause that completely rules out Covid-19, such as a fatal physical injury.”
- The same CBS news station reported in May about a death in Colorado where C-19 was completely ruled out, but the state counted it anyway:
- A man was found dead with blood alcohol content about twice the level that is potentially fatal, and Montezuma County Coroner George Deavers ruled that he died of alcohol poisoning.
- Colorado’s Department of Public Health and Environment classified the case as a C-19 fatality because the man tested positive for C-19 after his death.
- The coroner stated: “Yes, he did have Covid, but that is not what took his life.”
- In Florida during July:
- A local Fox news station asked Dr. Raul Pino, the health officer of Orange County, if two people in their twenties who had allegedly died of Covid-19 had any preexisting conditions. Pino replied: “The first one didn’t have any. He died in a motorcycle accident.”
- Two days after the news station published this story, Pino’s office said the case “was reviewed,” and the person “was taken off the list for Covid fatalities.”
- Officials of the Maricopa County, Arizona Public Health Department stated in August:
- “Even if it’s not listed on their death certificate, anyone who has a Covid-19 positive test within a certain period of when they died, is also counted as a Covid-19 positive death.”
- If a person dies in a car crash and tested positive for C-19 in the prior 60 days, “Yes, the death would be added” to the C-19 death tally because “it is important to understand who died WITH the disease even if the disease was not the CAUSE of death. Obviously, fatal accidents are a small subset of the total.”
Short of scrutinizing every alleged C-19 death or a truly representative sample of them, there is no way to tell how many cases like those above are part of the official tally. However, certain evidence suggests they are not a large portion of the total:
- Contrary to Birx’s statement in March, the CDC issued guidance in early April that states: “Not all conditions present at the time of death have to be reported—only those conditions that actually contributed to death.”
- The CDC posted that guidance on April 3 when the official C-19 death count was 5,443 people, or less than one-thirtieth of the current tally. Thus, whatever happened prior to then can’t have a major impact on the total.
- Some states instruct people who fill out death certificates to exclude C-19 if it didn’t play an active role in the fatality. Mississippi, for instance, says: “If Covid-19 was unrelated to the cause of death and not a contributing factor, it should not be included” on the death certificate.
On the other hand, the CDC’s guidance and other government policies still incentivize or stack the deck in favor of including C-19 on death certificates. For example:
- The state of Alaska instructs medical professionals to report C-19 deaths according to this standard: “Whether Covid-19 shortened a life by 15 years or 15 minutes; whether Covid-19 is an underlying or contributing condition, the virus was in circulation, infected an Alaskan, and hastened their death. This must be reported.” Given the impossibility of determining if C-19 shortened a life by 15 minutes, these instructions favor placing C-19 on the death certificates of people who died with or after C-19 but not necessarily from C-19.
- The CDC’s guidance for certifying C-19 deaths provides three examples of how to record them on death certificates, one of which involves an 86-year-old female who was never tested for C-19, had a debilitating stroke three years prior to her death, and passed on with “a high fever and severe cough after being exposed to an ill family member who subsequently was diagnosed with Covid-19.” The guidance states the “underlying cause of death,” or the pivotal factor that led to her death, should be listed as “Probable Covid-19.” However, many other diseases can cause a fever and cough, and a recent CDC study shows it is not uncommon for people to display symptoms of C-19 but test negative for it.
- The federal CARES Act, which became law in late March, pays hospitals a 20% premium for treating Medicare patients who are diagnosed with C-19. Until recently, a positive lab test for C-19 was not needed to obtain this money, but the federal government added this requirement in September “to address potential Medicare program integrity risks….” Note that C-19 need not appear on a death certificate for hospitals to receive these payments, so it may not influence decisions to include it.
- The Mississippi Department of Health states: “If the patient was a confirmed Covid-19 case, but Covid-19 contributed to but did not cause the death, such as stroke,” C-19 should be listed in Part II of the death certificate. This again favors placing C-19 on death certificates, for as the director of Illinois Department of Public Health said: If “someone has another illness, like heart disease, and then had a stroke or other event, it’s not as easy to separate that and say Covid didn’t exacerbate that existing illness.” Note that the CDC includes in its C-19 death tally all death certificates that mention C-19, regardless of whether it appears in Part I or Part II.
A breakdown of how many C-19 deaths appear in Part I versus Part II might shed considerable light on the issue of C-19’s lethality. This is because Part I of a death certificate “is for reporting the sequence of conditions that led directly to death,” while Part II is for “other significant conditions that contributed to the death, but are not a part of the sequence of conditions directly leading to the death.” Thus, Just Facts requested such data from the CDC on September 11 and is awaiting a reply.
Summary
Media outlets have persistently reported on the number of C-19 deaths while ignoring vital facts that place them in context. A simple example of this is that 2.8 million people die in the U.S. every year, including about 170,000 from accidents. Also of great import, accidents rob an average of 30.6 years of life from each of its victims, as compared to roughly 10.8 years for C-19. Yet in contrast, media outlets don’t continually publicize the running death tally from accidents.
This focus on the raw number of C-19 fatalities—combined with the fact that the very nature of the disease makes these figures uncertain—has spurred controversy over the accuracy of the CDC’s death count. Adding fuel to the fire, the statements and actions of some public officials show clear evidence of overcounting.
But even if the real death toll is 50,000 less than the 200,000 deaths currently reported by the CDC, this 25% difference would have little effect on key measures of the pandemic’s severity.
Consider, for example, the infection fatality rate, which is the portion of people who die after catching the disease. In early March, the World Health Organization announced that “about 3.4% of reported Covid-19 cases have died” and that “by comparison, seasonal flu generally kills far fewer than 1% of those infected.” This 3.4% figure was widely reported, and many media outlets criticized President Trump for saying, “I think the 3.4% is really a false number,” and “I would say the number is way under 1%.”
As it turned out, Trump was correct, and the Center for Evidence-Based Medicine at the University of Oxford now estimates that the infection fatality rate for C-19 is “somewhere between 0.1% and 0.41%.” This is well below 1%, just as Trump stated, and within range of the flu’s infection fatality rate of 0.15%. So even if C-19 deaths are overcounted by 25%, and this exaggerates the fatality rates by the same amount, they would still be 0.1% to 0.3%—or practically unchanged.
Likewise, the CDC’s current best estimates for the infection fatality rate range from 0.003% for people aged 0–19 to 5.4% for people aged 70 and above. Again, a 25% change in these figures would leave them in the same ballpark.
Thus, debates over the death count are a distraction from more informative measures like the odds of dying from C-19 for those who catch it. In this case, the highly publicized figure of 3.4% proved to be off by about a factor of 10. That is a major factor that truly informs the big picture.
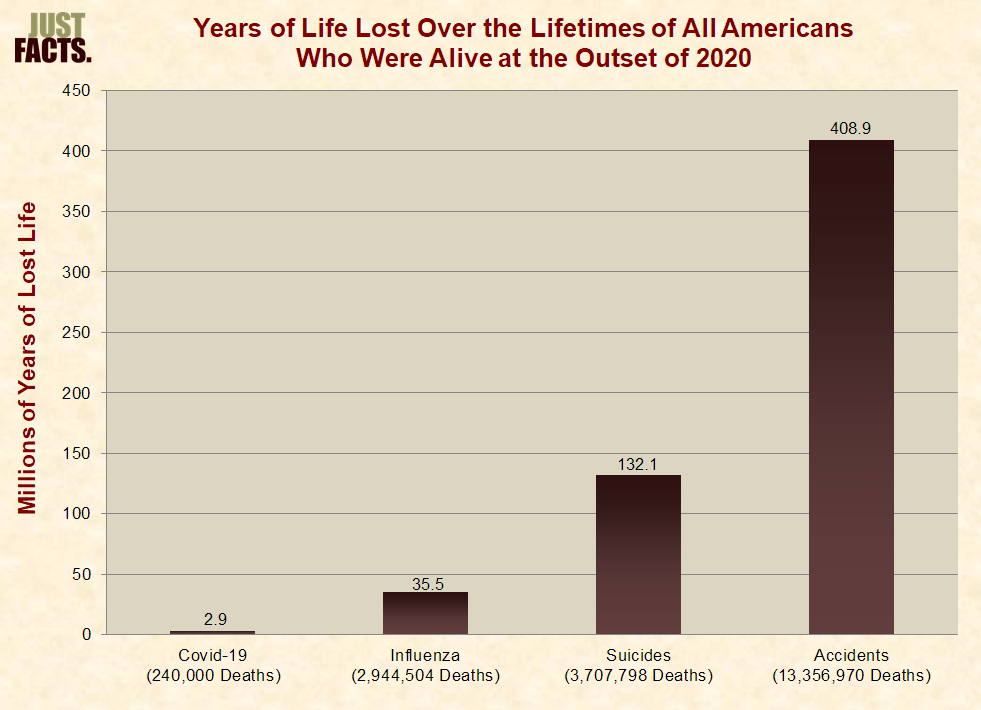
From an even broader perspective, the most comprehensive available measure of the threat posed by Covid-19 is the total years of life that it will rob from all people who were alive at the outset of 2020. This crucial measure accounts for the facts that:
- there is a material difference between a malady that kills a 20 year-old in the prime of her life and one that kills a 90-year-old who would have otherwise died a month later.
- Covid-19 is unlikely to have an ongoing high death toll because the virus that causes it mutates much less substantially than that of the flu and other contagious diseases. Thus, it is far less likely to keep taking lives in the face of acquired immunity and vaccines.
In the context of this broad measure, debates over the actual death toll amount to rounding errors in the relative threats posed by Covid-19 and other common scourges that take masses of lives every year:
In conclusion, the facts of this matter accord with a Government Accountability Office technology assessment published in July that found: “The extent of any net undercounting or overcounting of Covid-19 deaths is unknown.” More importantly, debates over the accuracy of this figure divert attention from other issues that have much greater implications for understanding the pandemic and how it should be addressed.
– – –
James D. Agresti is the president of Just Facts, a think tank dedicated to publishing rigorously documented facts about public policy issues.




Yes there is a virus out there that kills some people, and NO, it does not and never has been so deadly as to declare a pandemic or emergency to shut down this country and it’s economy.
Between China and the Democrats it’s all about getting Donald Trump out of the white house.
Why has it been necessary for so many lies to be told about Covid, Lies about who actually died because of Covid, rather than something else, Lies about the number of deaths, Lies about the prevention of covid, mask/no mask,
And most of all, Lies about a vaccine that was patent by China in 2019.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7054408
If you have any interest in knowing the full story about the virus, I’d suggest you visit both of these site, and the information they provide.
https://freedomheadlines.com/freedom-wire/former-employee-of-dr-fauci-blows-whistle-on-coronavirus-pandemic-video/
https://vaccineimpact.com/tag/dr-judy-mikovits
Pay particular attention to her comments about an “In-active virus” being injected in a vaccine and later a second injection that can active that virus.
Is this Bill Gates way of “Depopulating the earth” but blaming it on “bad vaccines”.
Too many lies, too much Politics are regulating this “disease”.
As long as there is a financial incentive for hospitals to report coronavirus Aspirus death then you will have exaggerated death counts. ,$13,000 for every coronavirus death, $35,000 if on a respirator ❗